

Abstract
Allogeneic stem cell transplantation (AlloSCT) is a curative option for acute myeloid leukemia (AML) patients. In first complete remission (CR1), young patients (< 60 years) with intermediate or unfavorable ELN disease risk are usually considered for AlloSCT. In contrast, because of the expected higher toxicity in older patients, the benefit of this treatment remains a matter of debate after 60 years, especially in the intermediate ELN risk group. In this multicenter analysis from the French Innovative Leukemia Organization (FILO), we investigated whether AlloSCT was beneficial for AML patients over 60 years old in CR1.
Inclusion criteria were: patients between 60 and 70 years of age diagnosed with AML from 2007 to 2017; CR1 after intensive chemotherapy; ELN-2010 intermediate or unfavorable risk group. AlloSCT was evaluated as a time dependent variable in survival calculations and in a multivariate Cox model adjusted on age, ELN group, transplantation period and stratified by transplantation center. We also used a multistate model as follow: initial state for all patients was "No Allo - CR" with time 0 at the time of CR. From initial state, patients can transit to "Allo-CR", or move through 2 absorbing states (non-relapse death (No Allo-NRM) or relapse (No Allo-Relapse). Similarly, once transplanted (i.e. in the state "Allo-CR"), patients can move to "Allo-Relapse" or "Allo - NRM" when such events occurred. The model allows the dynamic prediction of probability for a patient to be in a specific state considering specific initial state and time.
We analyzed 521 consecutive patients in 6 centers who matched inclusion criteria. Median age was 65 years (range: 60-70). ELN-2010 risk was intermediate and unfavorable in 376 (72%) and 145 (28%) patients, respectively.
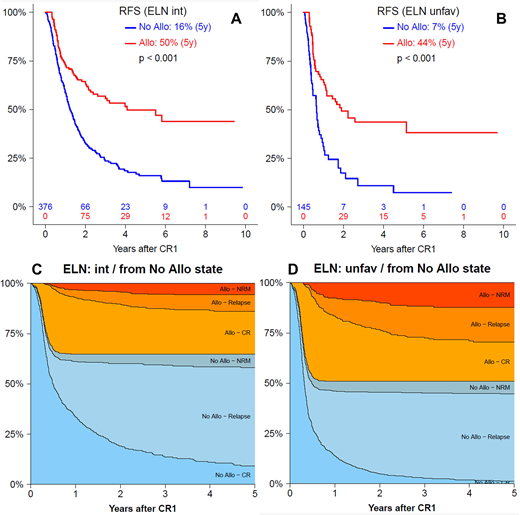
While all patients had a theoretical indication for AlloSCT in CR1, 199 (38%) were actually transplanted (129 (34%) and 70 (48%) in the intermediate and unfavorable risk group, respectively). In the whole cohort, AlloSCT as time-dependent variable significantly improved relapse-free survival ([RFS] at 5 years, No AlloSCT vs. AlloSCT: 14% vs. 47% p < 0.001) and overall survival ([OS] at 5 years, No AlloSCT vs. AlloSCT: 24% vs. 51% p < 0.001). In subgroup analysis based on ELN-2010 risk classification, AlloSCT significantly improved outcome of both ELN intermediate (No AlloSCT vs. AlloSCT: 5-y RFS: 16% vs. 50% p < 0.001; 5-y OS: 26% vs. 54% p < 0.001) and unfavorable (No AlloSCT vs. AlloSCT: 5-y RFS: 7% vs. 44% p < 0.001; 5-y OS: 17% vs. 46% p < 0.001) risk group patients (Figure A and B).
By multivariate time-dependent Cox model, AlloSCT significantly decreased the risk of relapse (HR [95%CI]: 0.29 [0.20-0.41] p < 0.001) and increased the risk of NRM (HR [95%CI]: 2.61 [1.38-4.94] p = 0.003). This led to a significant advantage for AlloSCT in both RFS (HR [95%CI]: 0.48 [0.36-0.64] p < 0.001) and OS (HR [95%CI]: 0.60 [0.44-0.81] p = 0.001). This benefit was observed in both intermediate and unfavorable ELN-2010 risk groups, with lower risk of relapse (intermediate: HR [95%CI]: 0.30 [0.19-0.46] p < 0.001; unfavorable: HR [95%CI]: 0.37 [0.19-0.72] p = 0.004) and better OS (intermediate: HR [95%CI]: 0.67 [0.47-0.96] p = 0.028; unfavorable: HR [95%CI]: 0.51 [0.29-0.91] p = 0.022).
Multistate model showed that 5 years after CR1, few patients were still alive in CR without AlloSCT (i.e. in the initial "No Allo-CR" state), whatever the ELN-2010 risk group (intermediate: 9%; unfavorable: 1% Figure C and D). Among patients who were transplanted, the probability for transiting to Allo-NRM state within 5 years post CR1 was 17% and 24% in intermediate and unfavorable ELN-2010 groups, respectively. Corresponding values for patients without AlloSCT transiting to No Allo-NRM state were 11% and 12%. Moreover, considering a landmark at 6 months after CR1, the multistate model showed that patients who received AlloSCT had lower probability of relapse at 5 years (22% and 33% in intermediate and unfavorable ELN-2010 groups, respectively) compared to those who did not (68% and 78% in intermediate and unfavorable groups, respectively).
AlloSCT for CR1 AML patients over 60 years of age is routinely feasible and significantly improves outcome in both intermediate and unfavorable ELN-2010 risk groups. Less than 10% of patients are long term disease free survival without AlloSCT, even in intermediate risk group, supporting that AlloSCT remains the first curative option for these patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal